When Cindy Kuikstra heard those words, she knew that her son, Andy Stuns, wasn’t just in serious trouble, but mortal danger. Stuns had been struggling with drug addiction for most of his adult life, and since he’d moved to Denver in 2014, he had been in and out of jail, busted for such crimes as stealing from department stores to finance his fixes. In May 2016, Stuns was about to be released from jail again when he called his mom to reveal that, right before going into lockup, he’d overdosed on heroin twice — only to be saved by the anti-overdose drug naloxone (market-branded as Narcan). Street drugs in Denver were becoming so potent and unpredictable, especially those laced with fentanyl, that Stuns didn’t think he’d last much longer before his next, potentially fatal overdose. He told his mom that he wanted to turn his life around before that happened.
Alarmed, Kuikstra purchased her son a bus ticket to where she lived in Michigan and sent him an extra $75 to spend on food during the journey.
Stuns never made it onto the bus.
Around 11:30 p.m. on May 17, 2016, a driver called 911 to report a man acting strangely on the sidewalk near the ambulance bay at Denver Health, near the intersection of Speer Boulevard and Bannock Street. When first responders reached Stuns, they recognized that he was experiencing a heroin overdose and rushed him inside the hospital, where doctors attempted to resuscitate him.
Stuns was pronounced dead at 12:01 a.m. on May 18, the day after his 28th birthday.
Kuikstra learned of her son’s overdose less than an hour after he died. Usually, it would take medical staff much longer to identify an individual who had no ID, but Stuns had been to Denver Health earlier on May 17 to pick up a number of prescriptions for other medical ailments he suffered from, including kidney failure; he was still wearing his hospital bracelet. “He must have used that $75 to get heroin,” Kuikstra muses. “And I’m guessing, based on where he was, that he used it right there in the hospital bathroom.”
Joelle Fairchild did not learn of her own son’s overdose quite as quickly. On October 23, 2014, she was informed that her son, 27-year-old Tony Fairchild, had succumbed to a heroin overdose on the Cherry Creek bike path a day earlier.
Rigor mortis had already stiffened parts of Tony’s body by the time first responders reached him.
A police detective told Joelle that a homeless man had called 911 around 8:45 p.m. on October 22 after seeing Tony sitting against a tree close to the 14th Avenue overpass, in the same unusual position he’d been in hours earlier. The lag led to an unsettling realization for Joelle: Because it was a warm evening, scores of cyclists and runners might have passed right by her son while he was dying.
Since those two young men overdosed in Denver, opioid- and heroin-related deaths have been on a precipitous rise. Earlier this month, the National Safety Council released a report documenting that opioid overdoses have officially surpassed vehicle crashes as the overall leading cause of death in the United States. According to the January 2019 report, Americans have a 1 in 96 chance of dying from an opioid overdose versus a 1 in 103 chance of dying in a vehicle crash.
Other statistics for what’s been dubbed “the opioid crisis” are equally staggering. In 2017, 72,000 Americans died from opioid overdoses. Of those, 1,012 were in Colorado, with 201 reported within the City and County of Denver. Even for families that haven’t been touched by tragedy personally, the toll is becoming impossible to ignore; increasingly, opioid-related deaths are happening in plain view. In 2017, 28 of the people who overdosed and died in Denver were found in public locations, including parks, the Denver Central library, business bathrooms and alleyways.
In the face of the mounting health crisis, both Cindy Kuikstra and Joelle Fairchild have become supporters of an idea that each initially thought was radical — even extreme. The mothers are using their sons’ stories to support a push for Denver to have the first official “supervised use site” in the United States.
Such sites (also known as supervised consumption sites or, in the case of IV drugs, safe injection sites) currently exist in twelve countries, but have never been sanctioned in the U.S. The idea is to allow people to bring drugs — including heroin, cocaine and meth — that they obtained through outside means into a sanctioned space and to use them under medical supervision, without fear of arrest.
While Denver is not the only U.S. city considering authorizing such a site — San Francisco, New York and Philadelphia are others — it moved to the forefront of the controversy in late November, after Denver City Council passed an ordinance paving the way for a supervised use site (SUS) in the Mile High City. Such a facility would also need state approval, so a bill will soon be introduced in the Colorado Legislature for consideration during the current session, which ends May 3.”As a service provider, I’m fucking tired of people I know and loved and served dying.”
tweet this
Opposition is already lining up. During House Republican Minority Leader Patrick Neville’s opening speech at the legislature on January 7, he drew a hard line in the sand: “Some well-intentioned people would have you believe this is a compassionate approach to a complicated problem. ... So-called safe injection sites are not the answer. Asking the taxpayer to foot the bill to continue addiction is a bad idea. Subsidizing the slow-motion suicide of our citizens is wrong. We can and must do better.”
According to state lawmakers who support the concept, any SUS in Denver or elsewhere in Colorado would involve no taxpayer money; such a site would be privately funded and staffed by a nonprofit. They also argue that the sites are not about condoning drug use; the facilities are intended to build relationships between users and service providers, who can offer treatment and recovery options if and when people who use drugs say they are ready for them.
More than anything else, though, the aim is to prevent deaths.
As mothers who lost their sons to drugs, both Kuikstra and Fairchild say they were initially shocked by the idea of supervised use sites: Allow people to use, just like that? But after studying up on SUS proposals — learning, among other things, that even with millions of visits to 102 such sites internationally, no one has ever died — they have become convinced that such a site could work in Colorado as part of a broader continuum of efforts around “harm reduction.” That’s the catch-all phrase used for strategies and ideas aimed at reducing the negative consequences associated with drug use, including the spread of preventable diseases such as hepatitis C and HIV.
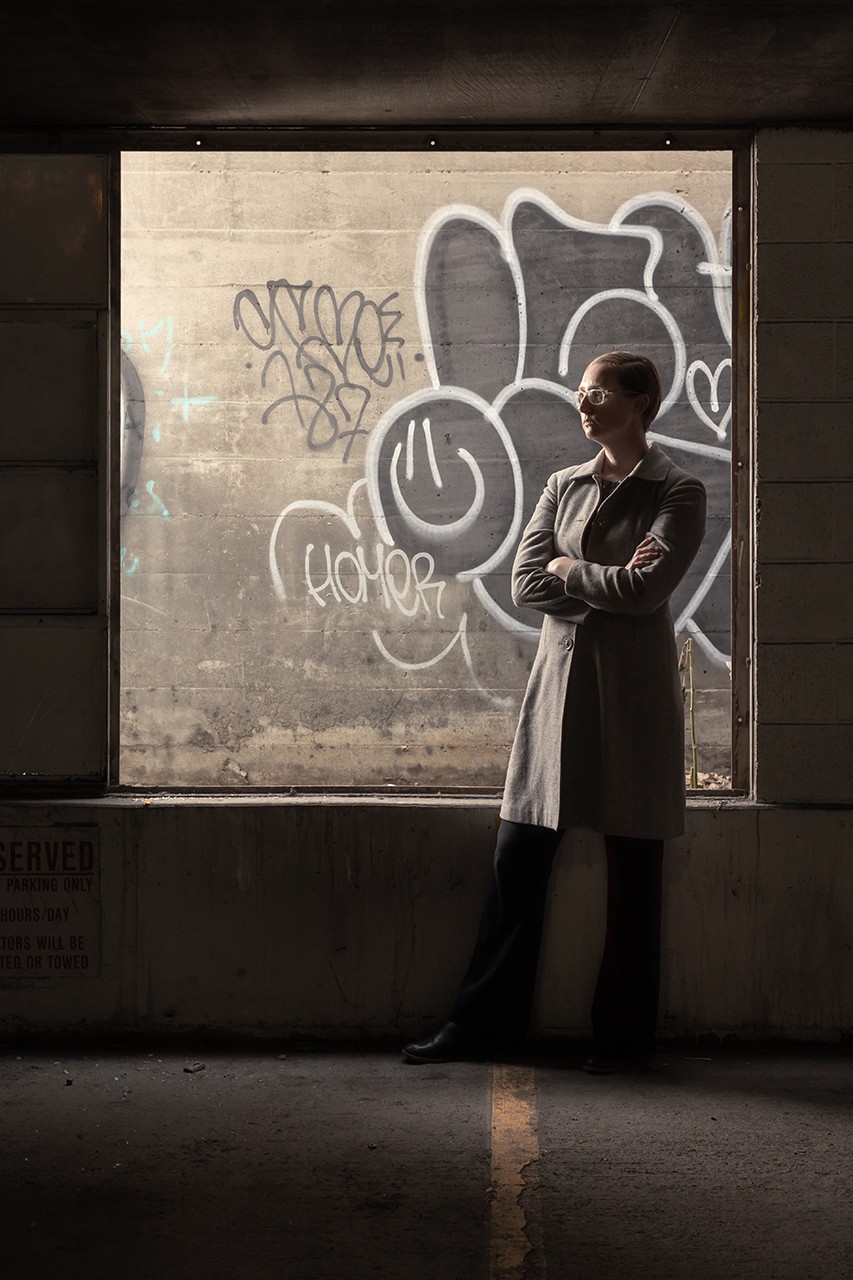
The person who helped rally their support was Lisa Raville of the Harm Reduction Action Center. As the director of Colorado’s largest syringe-access program, Raville has made supervised use sites her personal mission.
“As a service provider, I’m fucking tired of people I know and loved and served dying,” Raville declares. “I’m an action gal. And that’s why I don’t run a ‘harm reduction center.’ It’s a harm reduction ACTION center.”

Joelle Fairchild with a portrait of her son Tony next to the tree where he passed away.
Jake Holschuh
On a snowy Friday in early January, I’m driving Raville and her organization’s overdose prevention coordinator, Vernon Lewis, to different places where clients of the Harm Reduction Action Center have overdosed and died from drug use in Denver.
It’s a morbid tour — seeking out the spots where users, many of them young, spent their last moments — but Raville and Lewis insisted upon it. Raville, 39, sits in the passenger seat, bundled in multiple layers against the frigid temperatures, but her short hair and square, translucent-framed glasses poke out above her collar. Lewis is in the back seat, slight and compact.
Both work full-time at the Harm Reduction Action Center, the largest of Colorado’s ten syringe-access programs. Located across from the State Capitol in a one-story storefront squeezed between apartment complexes on East Colfax Avenue, HRAC opens its doors at 9 a.m. every day to between 120 and 150 people on average, who come to obtain sterilized equipment related to drug use — including clean needles — as well as check their mail, test street drugs for fentanyl, or request referrals to other programs in Denver that can help with housing, substance-abuse recovery and employment.
Since HRAC’s syringe-exchange program began in 2012, the nonprofit has served over 8,000 participants; in 2018, approximately 4,500 individuals visited HRAC to obtain sterile syringes, tourniquets, alcohol wipes, tubes of sterile water, metal heroin cookers and more. The supplies help prevent the spread of diseases such as HIV and Hep C.
More than half the staff are current or former injection drug users. “It’s important to reflect the community we serve,” says Raville. “Right now the Harm Reduction Action Center is that one safe space where people can come in and talk about their drug use. Every other place in town you have to be abstinent or promise to be abstinent to receive their services. We get to cut out a lot of that bullshit.”
A tight-knit community based on the principle of zero judgment has formed around HRAC, which was founded in 2002. And even though staffers don’t push treatment, they still keep track of each “ask” by individuals they serve who seek treatment or recovery options. There have been more than 41,000 asks so far, according to HRAC’s running tally.
But while all users who visit HRAC, even if it’s just to pick up a condom or an alcohol wipe, are being proactive about their health, they still cannot use there.
In Denver, black tar heroin is the most common opiate dealt on the streets; it’s melted, then injected because of its crude quality. “And we know the average heroin user injects three to five times a day,” Raville continues. “Meth users will do their thing one to two times a day. And cocaine users will use as much as fifteen times a day. The thing is, with heroin use or opioid use, over a period of time you’re no longer getting high, you’re doing a minus-withdrawal — which is like going from the pain of the flu times 1,000 to being normal or well again. You are just trying your best to stay out of withdrawal. So if you can’t find a bathroom, you’re going to go behind a dumpster, because you’re physically ill and need to get well again.”
At this point on the tour, we’re somewhere between the border of the Lincoln Park and Sun Valley neighborhoods, in the industrial area south of Mile High Stadium. “Turn here,” Raville says, directing me toward a train overpass.“Right now the Harm Reduction Action Center is that one safe space where people can come in and talk about their drug use."
tweet this
At the bridge, the three of us get out of the car and start walking along an access road paralleling the train tracks. Lewis says that the area has been frequented by homeless campers since the city passed its camping ban in 2012, forcing people to sleep in more hidden areas, and I do start seeing shopping carts, blankets and other evidence of encampments.
Raville sees something else.
“Oh, this would be a good place to inject!” she says brightly.
Raville is not a user, but she’s always trying to see things from her clients’ perspectives. If users don’t have a private space where they can inject, she explains, they will probably try to find a business bathroom. If that’s unsuccessful, they’ll look for a spot as hidden as possible — such as the access road we’re walking on. “When you see someone who’s injecting in an alley, that’s probably someone who tried to go into a business bathroom first and couldn’t, and so they’re behind a dumpster,” she says. “They’re probably rushed, looking over their shoulder to make sure a cop doesn’t come up on them. So they might not use an alcohol pad, and any time you break your skin, you’re at risk of an infection… .”
Further along the access road, we move under I-25; up and to our left is an elevated ledge shielded from the sky by an expanse of cold, gray concrete. RTD recently built a chain-link fence around the ledge to deter campers, but we notice a rope hanging from the fence, perhaps fifteen feet in length, with knots spaced out every few feet.
“This is where Angelina passed away,” Lewis says as we inspect the spot.
“Really?” says Raville.
“Yeah.”
Raville turns toward me. “Angelina was very well-liked in the community,” she explains. “She was super nice. Totally popular.”
Angelina was also one of six HRAC participants to die of a drug overdose in January 2017 alone. “Every day I called the coroner’s office, and every day they seemed to have somebody,” Raville recalls. “Participants’ hearts couldn’t take it, staffs’ hearts couldn’t take it… .”
Then, on February 3, 2017, a man was found dead in a bathroom stall of Denver’s Central Library; the 25-year-old had succumbed to a lethal combination of heroin, meth and two anti-anxiety medications. Television stations pounced on the story with sensational broadcasts, including a 9News investigation that followed up on the death with undercover footage of down-and-out men and women dealing and using drugs throughout the library. Much was made of the fact that the library had started to train its staff to carry and administer Narcan to reverse overdoses, a practice already reported by Westword that continues today.
The spike in overdose deaths sparked Raville’s crusade for a supervised use site, a controversial concept she’d heard about for years — including from an HRAC volunteer from Australia, which has such sites — but had hesitated to bring up with her board of directors. Besides, there were more pressing issues HRAC had to push through the legislature: syringe-exchange (2010), legal protections for people reporting overdoses to 911 (2012), expanding access to Narcan (2013 and 2015).
But in early 2017, she decided it was time to suggest supervised use sites. “I was also so tired of people yelling about finding syringes in high drug-trafficked areas and people injecting in bathrooms,” she says. “So at least now I could tell them, ‘Well, do I have a policy initiative for you!’”
In early 2017, the Denver city councilman who represents HRAC’s district, Albus Brooks, was also looking into supervised use sites...though Raville didn’t know it at the time.
Like so many others, Brooks started out as a skeptic. “It sounds outrageous and scandalous,” he acknowledges. “But I think once you start looking at evidence and you start thinking about it, you see how much it makes sense as part of the overall vision of harm reduction, treatment and prevention, and it’s hard not to become a believer.”
Brooks became a believer after he was diagnosed with chondorosarcoma, a rare form of skeletal cancer, in summer 2016 and underwent extensive surgery to remove a fifteen-pound grapefruit-sized tumor. “Afterward, I was given as much OxyContin as possible,” he recalls. “I actually became reliant. I experienced some withdrawals. I started acting erratic, not like myself. My mind wanted to be back at work, but my body was dragging. And I realized, as headstrong as I am, how close I was to becoming addicted. It was a transformative moment for me, realizing we all can fall into this trap of addiction.”
As Brooks was contending with his growing reliance on painkillers (he’s since gotten off them, though he had to undergo a second surgery to remove a smaller tumor in 2018), he was invited to a Democratic leadership conference in November 2016 that included a number of seminars on the opioid crisis. That’s when he first heard about supervised use sites, including an eyewitness account from Svante Myrick, the mayor of Ithaca, New York, who’d visited a state-approved operation in Vancouver called InSite, the first legal supervised use site in North America.
After a fierce fight to get the project up and running, mostly spearheaded by drug users, InSite started in 2003 as a small pilot program with limited hours on Vancouver’s east side, near an open-air drug market that’s been operating for decades. Today the nondescript storefront is open from 9 a.m. to 2 a.m. daily. In 2017, the facility recorded 175,464 visits by 7,301 unique users; many come several times a day.
Through the front door of InSite is a waiting room with a check-in area. Visitors share a small amount of information about themselves, including what drugs they’ve brought and their names (nicknames are fine); when the facility is ready, they’re invited into a back room with thirteen cubicles, each with a spotlight overhead and a needle disposal box attached to the side. As at Denver’s HRAC, there are sterile supplies, such as syringes, alcohol wipes and tourniquets, that participants can collect before they settle into a booth.
People are given anywhere from five to twenty minutes in a cubicle. If they want to consult a member of the medically trained staff, they can get advice about such things as dosage and optimal veins for injections, though staff members refuse to physically poke someone’s skin with a needle or push a plunger.
In the case of an overdose — 2,151 occurred at InSite in 2017 — staffers are trained to respond with a series of increasing interventions. During an overdose, the brain starts to shut down, losing the ability to control basic autonomic functions such as breathing. If staff members at InSite notice that a participant appears sleepy or unresponsive, they’ll first use their voice to try to get a response. Next, a staff member will knock on the desk to cause a vibration. If the user is still unresponsive, a staffer will try a hard squeeze to the shoulder. Continued unresponsiveness means it’s time to bring out an oxygen tank and give what’s known in the harm reduction community as “rescue breaths,” tilting the head back and delivering air to the overdosing person’s lungs. Naloxone is also administered if necessary.
Of all the overdoses at InSite, including the 2,151 recorded during 2017, not a single person has died. In fact, that’s true for all sanctioned supervised use sites around the world.
Even so, InSite faced an army of opponents when it was first proposed. Many worried about a so-called “honeypot effect,” that a supervised use site would draw in drug users from a wider geographic area, or that people from even farther afield would use it as a sort of tourist destination, treating the neighborhood as a lawless drug haven akin to “Hamsterdam” in the television series The Wire.
Vancouver’s police department and British Columbia’s Ministry of Health have both determined that those concerns were unwarranted: Crime has actually dropped around InSite, overall drug use and dealing in the area have not increased, and overdose deaths in public spaces close to InSite are down significantly.“Subsidizing the slow-motion suicide of our citizens is wrong. We can and must do better.”
tweet this
“I started putting this puzzle together,” Inspector Bill Spearn of the Vancouver Police Department told radio station WHYY. “It made sense to me that the reason the number of [public] overdoses had dropped significantly was because of InSite.”
(But while public overdoses are down, numbers do show that overall overdose deaths, the vast majority of which occur in private residences, are up significantly since 2015. A study the British Columbia Coroner's Service concludes that fentanyl, now a factor in more than 80 percent of overdose deaths in British Columbia, is responsible for the recent rise.)
A legal challenge against InSite for allowing drug use, which ultimately reached Canada’s Supreme Court, was struck down after the court ruled that closing InSite would actually undermine public health and safety in Vancouver.
In November 2017, Councilman Brooks traveled to Vancouver with state representative Leslie Herod, whose sister had struggled with drug addiction and who was also interested in seeing InSite. By now, both had talked with Raville, and they were inspired to push for a supervised use site in Colorado.
But first they had to deal with another challenge: a severe shortage of space in existing substance abuse treatment and recovery programs. “I can’t get anyone into treatment today,” Raville says, adding that interested clients often must wait for an opening.
Herod decided to first introduce Caring 4 Denver, a Denver ballot initiative to fund mental health and substance abuse treatment programs with a nominal sales-tax increase, which was passed by voters in November 2018. “We first needed to make sure there were more resources in Denver, so I pushed forward with Caring4Denver with supervised use in the back of my mind,” Herod says.
Meanwhile, Raville helped craft a supervised use bill that was introduced at the legislature in early 2018 but relegated to a Republican-controlled Senate kill committee that February. Knowing that the political makeup of the Statehouse could change after the November midterm elections, Raville and Brooks decided to instead push for legislation at the city level, then return to the Capitol if their efforts in Denver proved successful.
In January 2018, Brooks — then Denver City Council president — introduced the idea of a supervised use site to his colleagues. “The progressives on council — you can probably guess who they are — were immediately on board,” Brooks recalls with a chuckle. “Other councilmembers were a concern.”
As for the mayor’s office, he says, “they started getting cold feet when they saw me going on trips and actually doing community meetings; they also had a lot of concerns. So I realized I needed to organize this by myself and with Lisa [Raville] and the community.”
And organize they did.
Brooks sent out a pair of surveys targeting prominent community leaders and activists to gauge their support for a supervised use site. After reading through Brooks’s explanation, over 80 percent of the respondents said they were in favor, he recalls.
With his efforts, Brooks remained mindful of the history of the Drug War and how it has disproportionately affected people of color in America. “There are people in the African-American community who are concerned — as I’m concerned — about how in the ’80s we stigmatized people around the crack epidemic. And one of the things I wanted in our bill was to include all drugs, not just heroin, which is symbolic to say: This is what we should have been doing in the ’80s for individuals,” he explains.
Once the survey data was collected, Raville persuaded Brooks that they needed to get business owners on board with the proposal, especially those owners who have been dealing with users overdosing in their bathrooms.
The issue is significant. At some public facilities, such as RTD’s bus terminals, facility managers have simply removed stall doors or installed “security doors” that allow anyone to look into a stall to check on its occupants. Raville knew that plenty of businesses were struggling with overdoses in their restrooms, too, only the owners didn’t have a central place to talk about the problem or learn about alternative solutions.
When it came time for city council’s consideration of supervised use sites, she knew just who to ask to testify.
Dan Scales, who’d opened a pharmacy next to Benedict Fountain Park on 20th Avenue in 2014, had personally witnessed two overdoses at his business. He already knew Raville from helping her with legislation expanding access to Narcan that passed the legislature in 2015, and agreed to provide a business owner’s view of opioid overdoses.
Scales and his staffers had witnessed one overdose death even before the pharmacy opened. The group had met outside the building while it was under construction and were about to carpool to tour a primary wholesaler when they noticed a pale-looking man shaking on the sidewalk. “He didn’t look right, so I gave him a tap on the shoulder,” Scales recalls. “I realized he was OD-ing, so I did CPR on him for a few minutes. Then the paramedics showed up. But it was apparent as soon as we started CPR that he was pretty far gone.
“We carried that around with us for a while,” Scales continues. “I’d say more myself than my staff. I wish I’d been there a few minutes earlier, but you can’t really beat yourself up about it, and now I think we’ve done as much as we can to make sure it doesn’t happen again.”
All of Scales’s pharmacists have been trained to administer naloxone, through a program that Raville and Lewis run at HRAC. Scales himself had to do that about eighteen months ago, when he noticed that a young man had been in his pharmacy’s bathroom for an unusually long time. “I knocked to check, then found him collapsed on the floor in the bathroom,” Scales says."I think we’ve done as much as we can to make sure it doesn’t happen again.”
tweet this
Scales ended up saving the man from overdosing on heroin by administering naloxone. “After that specific incident, I had a lot of trouble justifying allowing open access to our bathrooms,” he adds. “I was the one that identified that a person had been in there too long and found him on the floor. But what if nobody noticed and one of my employees walked in on a body?”
To avoid such tragedies, he’s joined those pushing for a space that gets use into a safer environment. “For everything that we put into helping people overcome addiction, some people are ready and some people aren’t,” he explains. “And for those who aren’t, you want to at least make sure they’re safe. And if you want to make sure they’re safe, you have a couple options: You can watch them, or you have someone else watch them. And if you want to be the one in charge, are you trained and prepared? If you’re not, you’re doing the community a disservice by shutting the door without opening another one that’s an alternate. You’re not condoning drug use or recommending that people take drugs. You’re allowing it to happen in a safer environment for those that are already going to.”
Erika Righter, who runs the socially conscious boutique Hope Tank on Broadway, has dealt with similar issues. “We had to make our bathroom no longer accessible because I had one incident when someone definitely was in there and was having some issues. But my staff is not trained and prepared for crisis management,” she says. “Staying in isolation is what’s killing people, because they’re OD-ing alone. But shame and isolation does not make people better. Right now, this is a huge drain on our community. If you look at it from a human perspective, this is a massive loss of talent. We need to shift people’s perspectives of who these drug users are. Many of them are probably your friends and family who can be high-functioning on these drugs but also in tragic pain. I think that’s part of what Lisa and the Harm Reduction group is doing well: putting a different face to this. And while [a supervised use site] is not a silver bullet, this is certainly one tool.”
Scales and Righter were among dozens of business owners who signed a letter of support for Brooks’s proposal; both testified before Denver City Council in November.
Even Brooks was surprised by the final council vote: 12 to 1, with Kevin Flynn supplying the only no vote.
Explaining his position, Flynn noted how police officers and other institutions around the city, including the library, are now carrying and administering naloxone to reverse overdoses when they encounter them. Rather than a central, supervised site, he advocates for more dispersal of the anti-overdose drug through a community naloxone distribution program, such as one currently running in Salt Lake City.
But Cathy Alderman of the Colorado Coalition for the Homeless, which supports a supervised use site, says the city shouldn’t be relying ever more heavily on community members, including police officers, to reverse overdoses.
“We need to stop relying on our police force to be our health providers — that’s not their job,” Alderman says. “And ultimately there’s a conflict there, too, since the use of these substances is often illegal. So if you’re going to be charging somebody with use or possession in public but also trying to save them with naloxone, you’re not really going to be able to address the substance use disorder at its core. And I think that’s what we’d like to see: How do we actually help people out of these addictions?”
Addressing addictions is Brooks’s ultimate goal, especially with the expanded treatment options expected to come out of Caring 4 Denver.
Any proposed supervised use site still faces a major obstacle: The use of Schedule I drugs is illegal at the federal level.

It took the feds less than a week to send their response to Denver’s ordinance after it passed city council. On December 4, the U.S. Attorney’s Office for Colorado and the Denver Field Office of the Drug Enforcement Administration issued a scathing letter that, in no uncertain terms, threatened “forfeiture of the property, criminal fines, civil monetary penalties up to $250,000, and imprisonment up to 20 years in jail for anyone that knowingly opens, leases, rents, maintains, or anyone that manages or controls and knowingly and intentionally makes available such premises for use.”
The letter continues: “Just like so-called crack houses, these facilities will attract drug dealers, sexual predators, and other criminals, ultimately destroying the surrounding community. More importantly, the government-sanctioned operation of these facilities serves only to normalize serious drug usage — teaching adults and children alike that so-called ‘safe’ drug usage is somehow appropriate or can actually be done ‘safely.’ The type of drug use contemplated here is always life-threatening behavior.”
But supporters of supervised use sites have remained steadfast. Leslie Herod compares the letter’s fighting words to threats Colorado received as it considered legalizing recreational marijuana. “The feds were on us then, but we went forward, and look, the sky has not fallen,” she says.
Senator Brittany Pettersen, who will introduce the SUS bill in the Colorado Senate this session, says she’s also undeterred by federal intimidation. “We have the legal authority to move forward during a public health crisis,” she says. “We have an emergency, and we’re able to act accordingly at the state and local level.”
For Pettersen, that emergency hit home long ago. Her mother struggled with opioid addiction for years and overdosed, as Pettersen puts it, “too many times to count.”
Her soon-to-be-introduced bill, which she promises will have a Republican co-sponsor, is not prescriptive, she says; it won’t require any supervised use sites in Colorado. “It’s simply going to allow local governments to determine how they want to address the opioid epidemic and if this is the right option for them,” she explains.
“Look, I wouldn’t want to think of my mom going to a place like this. I want to think of her being sober,” Pettersen continues. “But I’m the last person in the world who would ever pass anything that would increase drug use, because it has destroyed our family and created pain in our lives. I know firsthand how damaging addiction can be and how bad it can get.”
"I know firsthand how damaging addiction can be and how bad it can get.”
tweet this
But Pettersen will have to get her message through many opposing voices, which seem to be amplifying in volume and number as the SUS bill gets closer to becoming a reality. Increasingly vocal critics include Denver radio station KNUS hosts Peter Boyles and Steffan Tubbs, who traveled to Vancouver earlier this month on their own “fact-finding” mission to give on-the-ground reports about drug use around supervised use sites in the Canadian city. KNUS even has a page on its website dedicated to opposing supervised use sites.
Denver Mayor Michael Hancock, who is currently seeking re-election in May, is certainly aware of all the chatter around supervised use sites. In November, he released a statement saying he fully supported the bill passed by Denver City Council. But on January 16, he told 9News’s Kyle Clark that he was “not necessarily” committed to the idea of supervised use sites, causing the television station to proclaim that the mayor was “walking back” his support.
Pressed for clarification, Michael Strott, the mayor’s deputy communications director, wrote in an email that Hancock still supports the bill passed by city council and his position “hasn’t shifted from when he signed it.”
Hancock also provided the following statement: “Like cities across the country, Denver is seeing significant numbers of people dying each year of drug overdoses. As a city, we need to look for innovative answers. While we still have significant legal, implementation and community outreach concerns and details to work out, as well as state legislative action to even begin to pilot this approach, I fully support new approaches to address this crisis.”
Among those new approaches: The City of Denver and the Colorado Attorney General’s Office have joined other municipalities and states in filing suit against pharmaceutical companies that manufacture opioids; in fact, Denver filed a second such suit in January. The hope is that companies such as Purdue Pharma — which sells OxyContin — will be forced to pay for some of the effects of the opioid crisis if it can be proven that the corporations engaged in deceptive marketing practices that flooded the market with dangerous drugs.
But for supporters of supervised use sites, if the goal is to have local governments decide on whether to host one, why is state approval needed at all? Currently, Colorado’s drug laws are similar to federal laws in that they don’t allow any on-site use of Schedule I drugs under penalty of arrest and asset forfeiture.
Herod and Pettersen will have their work cut out for them persuading their colleagues in the legislature, especially Republicans across the aisle, to support such a bill. And then there’s the looming question of what Jared Polis will do. The new governor has refused to take a stance on supervised use sites, even when prodded by pesky reporters.
Pettersen and Herod are cautiously optimistic.
“I think that Jared Polis is someone who’s tactical and innovative, and he’s going to analyze bills based on outcomes,” Pettersen says. “This is someone who leads, who comes out for or against things based on what he thinks is good for our state. And I think the numbers are clear across the world: This is a real solution.”

Senator Brittany Pettersen and Councilman Albus Brooks are fighting for supervised use sites at the state and local levels.
Jake Holschuh
Lewis was also something of a guardian angel for IV drug users: To date, he says, he’s personally saved 136 people from overdoses. He keeps a running count.
Some of those saves occurred after he was hired in 2015 by Raville as HRAC’s overdose prevention coordinator and he secured housing, but far more occurred earlier, when he lived on the streets. “People used to literally drive up and drop people off by my tent here,” he says, gesturing to an area next to an RTD train track. “Other times they’d carry people to the edge of camp and yell, ‘Vernon!’”
Lewis’s reputation for reversing overdoses grew once people realized that he knew how to administer “rescue breaths” to get oxygen to people’s lungs, as well as how to use Narcan. He made sure to have at least ten doses of Narcan on him at all times, picking them up from HRAC, where he’s been involved since 2009.
The stories of so many rescues have started to run together, he says, though some remain more memorable than others. “One time we were in this building here,” he says, as we turn a corner and walk by a boarded up two-story structure on Lipan Street, “and someone literally threw this chick who was OD-ing through the window so I could help her.”
But what’s most remarkable — and doesn’t seem remarkable at all to Lewis — is that he and some of his friends ran their own, unofficial supervised use site in another boarded-up building by the Sixth Avenue viaduct.
“Oh, yeah, that was totally a supervised use site!” Raville interjects as Lewis describes how, in that building, at least one person who was trained in the use of Narcan would stay sober and monitor others as they used drugs to make sure nobody overdosed. It took discipline and trust, but Lewis and his friends stuck to the system.
“So...do you think that was successful?” I ask.
“Well,” Lewis responds. “No one died.”

Andy Stuns wanted to leave Denver before experiencing his next overdose.
Courtesy of Cindy Kuikstra
“If there was such a [supervised use] site when Tony was still alive, I know he would have used it, and it could have saved his life,” Joelle says.
Tony was a lover of the outdoors, music and art, who helped others and did not judge. Andy played drums in high school and was on the dive team. He took third place at a state wrestling competition and loved snowboarding and skateboarding.
Both made efforts to fight their addictions but just needed more time. And help.
Joelle found out that her son had been a member of HRAC in 2015. In preparation for Overdose Awareness Day that year, she took a picture of Tony to HRAC’s Colfax storefront, and staff members recognized him.
Kuikstra had actually been to HRAC before her son died; in 2014, during one of his stints in jail, he’d asked her to come to Denver when he was released and get him to a treatment center run by the Salvation Army. Before he checked in (he did not make the full thirty days under the organization’s zero-tolerance drug policy), Stuns took her to the Harm Reduction Action Center.
“I think it was important for him to show me what goes on there,” Kuikstra recalls. “He felt loved and accepted there, and it was a place for him to go and relax.”
While they were at HRAC, Stuns showed his mother the center’s “memorial wall,” which includes portraits of former participants who died of drug overdoses.
“Andy,” Kuikstra told her son. “I don’t ever want you to be on that wall.”
“I know, Mom,” he replied.